Empowering dialysis users and caregivers
Search for dialysis centres here
 Log in to explore the world's most comprehensive database of dialysis centres for free!
Log in to explore the world's most comprehensive database of dialysis centres for free!
| Advances in immunotherapy for renal cell carcinoma - ScienceBlog.com (blog) |
 |
 |
|
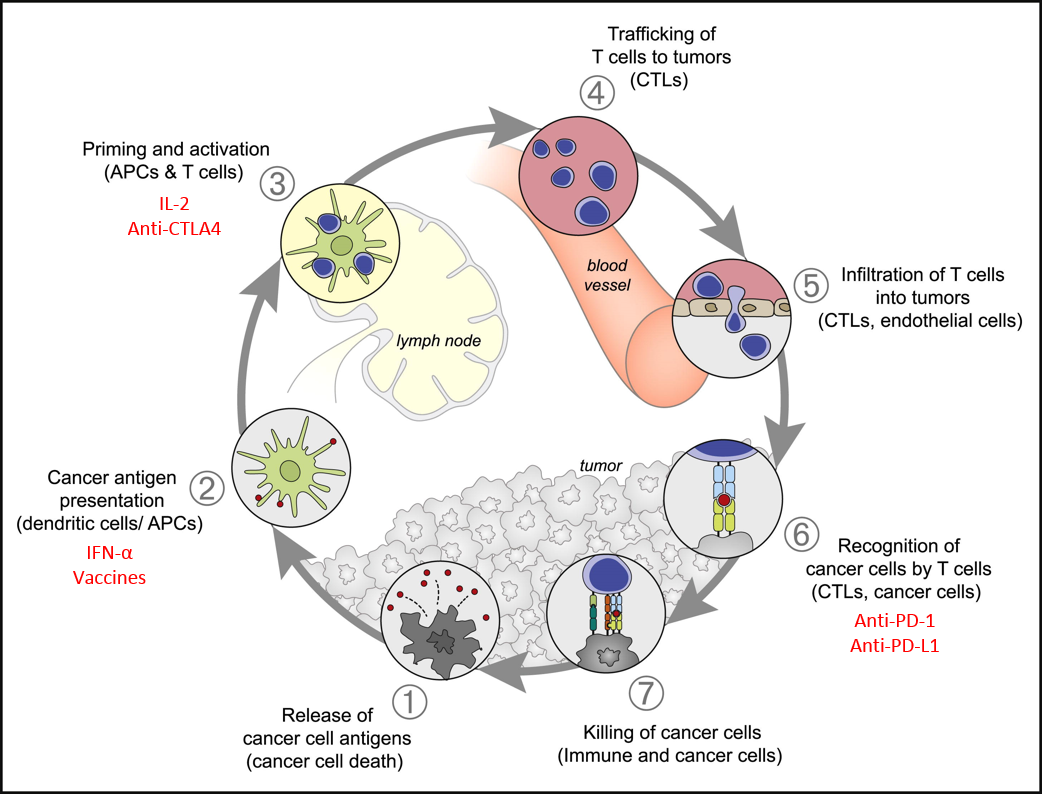
In recent years there has been renewed interest in immunotherapies to treat of metastatic renal cell carcinoma (mRCC). Immunotherapies increase the body’s natural finely regulated multiple-step anti-tumour immune response (Figure 1). The balance of stimulatory and inhibitory signals (reviewed in Chen & Mellman, 2013) are important in maintaining self-tolerance and modulating normal immune responses to minimising health tissue damage. However, tumours can develop mechanisms to evade this immune response. Figure 1: Immune Response Cycle. The major steps in the immune response cycle to cancer cells. Immunotherapies target a number of different steps (red). Modified from Chen & Mellman (2013) Immunity 39, 1-10.The approved immunotherapies for RCC are the cytokines Interferon-alpha (IFN-?) and Interleukin-2 (IL-2) to stimulate T-cell activity. Unfortunately this can result in a variety of treatment related toxicities. The response rate to these drugs is relatively low but the responses are more likely to be durable. An alternative strategy is to inhibit specific immune checkpoints that normally act to limit excessive immune activity. The numerous stimulatory and inhibitory checkpoints in the immune system minimise the death of healthy, “self” cells in an immune response. The presence of inhibitory signals on tumour cells can therefore stop an immune response but the blockade of these inhibitory signals can increase the immune response and tumour cell death. A list of ongoing trials is available here. One such inhibitor is Cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) which when bound to B7-1 or B7-2 disrupts early T-cell activation and blocks cytokine production. Ipilumumab binds to CTLA-4 and blocks this inhibition resulting in increased production of auto-reactive T-cells and cytokines. While some patients have responded well to ipilumumab there are some severe adverse events (AE) associated with off-target effects of this drug (Yang et al., 2007). A different checkpoint target is the Programmed cell Death-1 (PD-1)/PD-L1 inhibitory signalling pathway which reduces T-cell signalling and activation helping to maintain peripheral tolerance. Anti-PD-1 antibodies – nivolumab, pembrolizumab and pidilizumab – and the anti-PD-L1 antibody MPDL3280A are effective at blocking this signalling. PD-1 is expressed on a range of immune cells and PD-L1 can be expressed by tumour cells minimising the immune response. Nivolumab is the most frequently used anti-PD-1 in RCC and early phase trials have shown enhanced long-term survival (Lipson et al., 2013), with varied doses of nivolumab inducing comparable response rates with manageable toxicity profiles (Motzer et al.,2015). There are also numerous ongoing trials investigating pembrolizumab which showed some response in melanoma patients but can have severe AE (Martin-Liberal et al., 2015). An alternative, and potentially complimentary, approach would be the use of cancer vaccines to prime the immune system for response to cancer cells. The introduction of antigen presenting cells (APCs) loaded with tumour-derived RNA, such as AGS-003, induces a tumour-specific immune response (Amin et al., 2015). A synthetic vaccine, IMA901, consists of 10 Tumour Associated Peptides (TUMAPs) bound to HLA ligands for presentation to the immune system and as in early trials (Bedke & Stenzl, 2013). The immune related AEs (irAE) seen in immunotherapy drug trials can differ from AE from other drug types and can be severe (Weber et al., 2012). Early diagnosis and effective toxicity management is required to ensure ongoing treatment is tolerable. Early trials suggest a correlation between response rate and frequency of irAEs and perhaps such irAEs could be worth enhanced survival. Further trials will also determine any risk of sequential toxicities that could impact on treatment regimens. In addition to the development of therapies there is also a great need for research into relevant biomarkers; currently there are only indicative and not predictive biomarkers to determine which patients are most likely to response. Patient selection could also reduce the use of ineffective treatments which have a high irAE risk but no or minimal health benefit. Patient fitness and toxic burden also needs to be considered as frailer patients may not be able to tolerate AEs or to survive an initial decline before response begins. As immunotherapies develop they may also be beneficial as adjuvant treatments following surgical resection. The responses to immunotherapies can be durable, continuing long after treatment has completed indicating the formation of tumour specific immune memory; they could therefore also be useful in reducing recurrence risk in high risk patients such as those with hereditary forms of RCC.
|