|
The potential use of BH3-mimetics to overcome apoptosis-resistance in renal ... - ScienceBlog.com (blog) |
|
Renal cell carcinoma (RCC), as well as other solid tumours, can prove resistant to standard cancer treatments such as chemotherapy. One mechanism likely to play a role in this resistance is activation of HIF signalling either as a result of hypoxia within the tumour or as the result of mutations as in BHD, VHL and TSC. Increased HIF activity, as well as altered PI3K/AKT/mTOR, MEK/ERK and TGF? signalling, can shift the balance of anti- and pro-apoptotic factors enabling tumour cells to survive in unfavourable conditions.
In response to cell death signals BH3-only family members, such as BIM, bind to and sequester the anti-apoptotic BCL-2 family members, liberating the pro-apoptotic BAX and BAK proteins that induce apoptosis (Figure 1). However, tumour-specific loss of BIM, and associated resistance to apoptosis, has been reported in several tumour types: in clear cell RCC samples (35/45) with a correlation between BIM expression and apoptosis-susceptibility identified in RCC lines (Zantl et al., 2007); in BHD tumour samples (Cash et al., 2011) and VHL-deficient cell lines (Guo et al., 2009) suggesting a role for FLCN and pVHL in BIM expression and stability respectively; and in breast cancer tumour lines with aberrant PI3K/AKT/mTOR or MEK/ERK signalling (Faber et al., 2011).

Figure 1: BIM binds to and sequesters Bcl-2 and Mcl-1 to induce apoptosis via dimerisation of BAX and BAK.
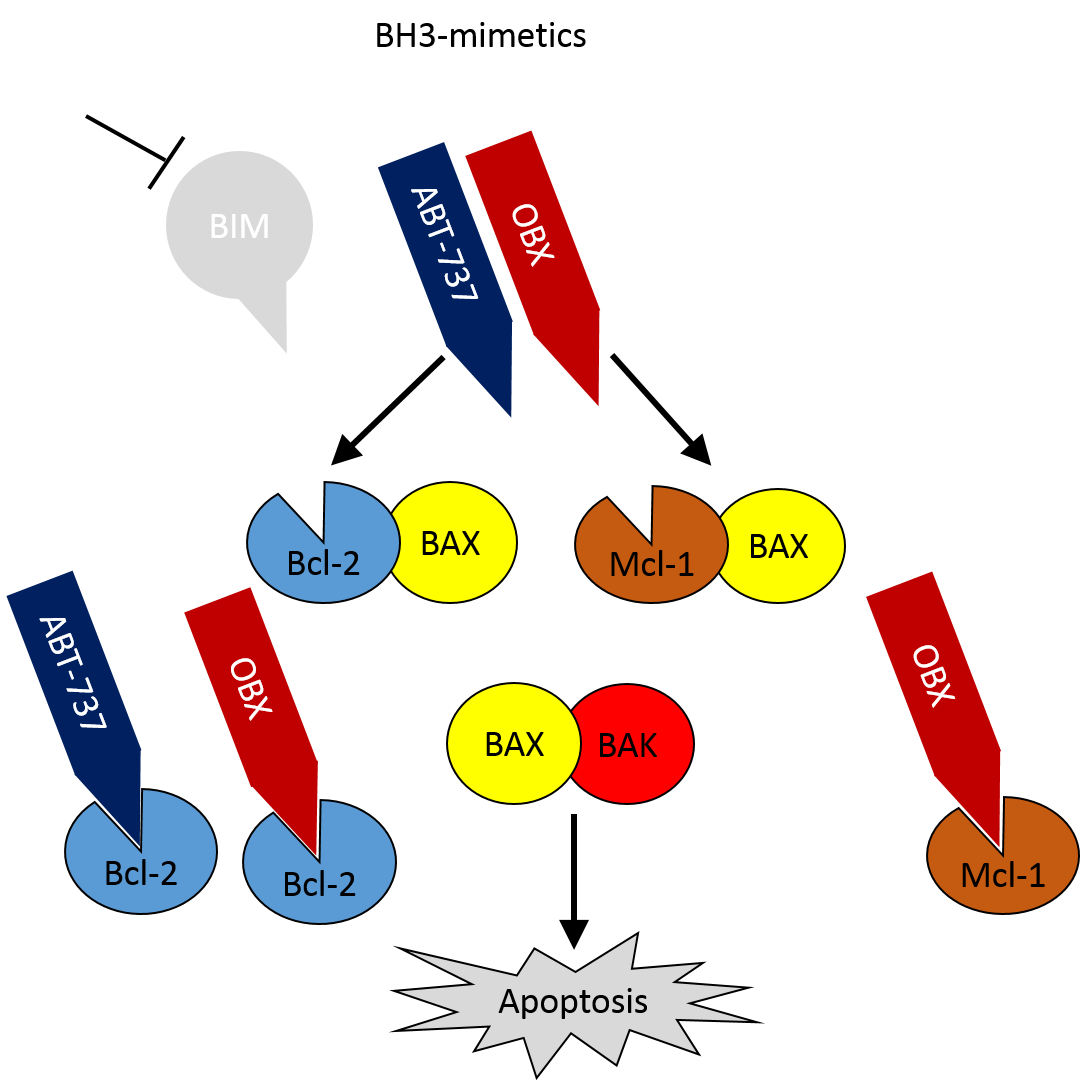
One potential treatment for such tumours is the use of BH3-mimetics – small molecule inhibitors, such as ABT-737 (or the orally bioavailable formulation ABT-263) and Obatoclax (OBX), which bind to BCL-2 and induce apoptosis (Figure 2, Oltersdorf et al., 2005, Tse et al., 2008, Nguyen et al., 2007). OBX has a broader specificity that ABT-737 binding MCL-1 as well as BCL-2, making it a more potent antagonist. Additionally it has been shown that OBX can reduce mTOR activity in melanoma cells (Espona-Fiedler et al., 2012) and both disrupt HIF-1-? protein synthesis and enhance proteosomal degradation to lower HIF-1? protein levels under hypoxic conditions (Gariboldi et al., 2015). As HIF signalling is often perturbed in RCC this suggests that the use of BH3-mimetic may also be useful in these cases.

Figure 2: BH3-mimetics can bind Bcl-2 and Mcl-1 to induce apoptosis in the absence of BIM.
BH3-mimetics could be of particular interest in BHD as several of the pathways known to be altered in FLCN-deficient cells have been implicated in the control of BIM expression: increased HIF-signalling plays a role in BHD renal and pulmonary pathology (Preston et al., 2011, Nishii et al., 2013); increased mTOR activity has been seen in patient samples and BHD models (Baba et al., 2008, Nishii et al., 2013); and increased activation of ERK1/2 signalling was identified in FLCN-null kidneys (Baba et al., 2008).
In addition to these pathways Cash et al., (2011) reported a TGF?-dependent reduction in BIM expression and increased apoptotic resistance in Flcn-/- ES cells, with Flcn-restored cells showing rescued apoptotic response. A role for FLCN in the regulation of TGF? signalling had previous been suggested (Hong et al., 2010) following the reduction in TGF?-target expression in FLCN-null cells (including SMAD7 as discussed in a previous blog regarding a role of MMPs in BHD). Cash et al. determined that the deregulation of TGF? signalling resulted in hypoacetylation of target promotors, including BIM, and reduced expression. Treatment of these cells with either ABT-737 or an HDAC inhibitor increased susceptibility to apoptosis identifying them as potential therapies in BHD.
BH3-mimetics have proven successful in a range of cancers and there are several ongoing trials assessing the efficiency of ABT-263 and OBX in the treatment of solid tumours. The reduction in BIM expression in BHD tumours and the links between FLCN-associated signalling and BIM expression suggest that BH3-mimetics could be a valid treatment in BHD. Interestingly Cash et al. reported a reduction in BIM levels in a fibrofolliculoma sample raising the possibility for BH3-mimetics to be used for multiple BHD phenotypes.
- Baba M, Furihata M, Hong SB, Tessarollo L, Haines DC, Southon E, Patel V, Igarashi P, Alvord WG, Leighty R, Yao M, Bernardo M, Ileva L, Choyke P, Warren MB, Zbar B, Linehan WM, Schmidt LS (2008). Kidney-targeted Birt-Hogg-Dube gene inactivation in a mouse model: Erk1/2 and Akt-mTOR activation, cell hyperproliferation, and polycystic kidneys. J Natl Cancer Inst. Jan 16;100(2):140-54. PubMed PMID: 18182616.
- Cash TP, Gruber JJ, Hartman TR, Henske EP, & Simon MC (2011). Loss of the Birt-Hogg-Dubé tumor suppressor results in apoptotic resistance due to aberrant TGF?-mediated transcription. Oncogene, 30 (22), 2534-46 PMID: 21258407.
- Espona-Fiedler M, Soto-Cerrato V, Hosseini A, Lizcano JM, Guallar V, Quesada R, Gao T, Pérez-Tomás R (2012). Identification of dual mTORC1 and mTORC2 inhibitors in melanoma cells: prodigiosin vs. obatoclax. Biochem Pharmacol. Feb 15;83(4):489-96. PubMed PMID: 22155350.
- Faber AC, Corcoran RB, Ebi H, Sequist LV, Waltman BA, Chung E, Incio J, Digumarthy SR, Pollack SF, Song Y, Muzikansky A, Lifshits E, Roberge S, Coffman EJ, Benes CH, Gómez HL, Baselga J, Arteaga CL, Rivera MN, Dias-Santagata D, Jain RK, Engelman JA (2011). BIM expression in treatment-naive cancers predicts responsiveness to kinase inhibitors. Cancer Discov. Sep;1(4):352-65. PubMed PMID: 22145099.
- Gariboldi MB, Taiana E, Bonzi MC, Craparotta I, Giovannardi S, Mancini M, & Monti E (2015). The BH3-mimetic obatoclax reduces HIF-1? levels and HIF-1 transcriptional activity and sensitizes hypoxic colon adenocarcinoma cells to 5-fluorouracil. Cancer letters PMID: 25979228.
- Guo Y, Schoell MC, Freeman RS (2009). The von Hippel-Lindau protein sensitizes renal carcinoma cells to apoptotic stimuli through stabilization of BIM(EL). Oncogene. Apr 23;28(16):1864-74. PubMed PMID: 19305426.
- Hong SB, Oh H, Valera VA, Stull J, Ngo DT, Baba M, Merino MJ, Linehan WM, Schmidt LS (2010). Tumor suppressor FLCN inhibits tumorigenesis of a FLCN-null renal cancer cell line and regulates expression of key molecules in TGF-beta signaling. Mol Cancer. Jun 23;9:160. PubMed PMID: 20573232.
- Nguyen M, Marcellus RC, Roulston A, Watson M, Serfass L, Murthy Madiraju SR, Goulet D, Viallet J, Bélec L, Billot X, Acoca S, Purisima E, Wiegmans A, Cluse L, Johnstone RW, Beauparlant P, Shore GC (2007). Small molecule obatoclax (GX15-070) antagonizes MCL-1 and overcomes MCL-1-mediated resistance to apoptosis. Proc Natl Acad Sci U S A. Dec 4;104(49):19512-7. PubMed PMID: 18040043.
- Nishii T, Tanabe M, Tanaka R, Matsuzawa T, Okudela K, Nozawa A, Nakatani Y, Furuya M (2013). Unique mutation, accelerated mTOR signaling and angiogenesis in the pulmonary cysts of Birt-Hogg-Dubé syndrome. Pathol Int. Jan;63(1):45-55. PubMed PMID: 23356225.
- Oltersdorf T, Elmore SW, Shoemaker AR, Armstrong RC, Augeri DJ, Belli BA, Bruncko M, Deckwerth TL, Dinges J, Hajduk PJ, Joseph MK, Kitada S, Korsmeyer SJ, Kunzer AR, Letai A, Li C, Mitten MJ, Nettesheim DG, Ng S, Nimmer PM, O’Connor JM, Oleksijew A, Petros AM, Reed JC, Shen W, Tahir SK, Thompson CB, Tomaselli KJ, Wang B, Wendt MD, Zhang H, Fesik SW, Rosenberg SH (2005). An inhibitor of Bcl-2 family proteins induces regression of solid tumours. Nature. Jun 2;435(7042):677-81. PubMed PMID: 15902208.
- Preston RS, Philp A, Claessens T, Gijezen L, Dydensborg AB, Dunlop EA, Harper KT, Brinkhuizen T, Menko FH, Davies DM, Land SC, Pause A, Baar K, van Steensel MA, Tee AR (2011). Absence of the Birt-Hogg-Dubé gene product is associated with increased hypoxia-inducible factor transcriptional activity and a loss of metabolic flexibility. Oncogene. Mar 10;30(10):1159-73 PubMed PMID: 21057536.
- Song JH, Kandasamy K, Zemskova M, Lin YW, Kraft AS (2011). The BH3 mimetic ABT-737 induces cancer cell senescence. Cancer Res. Jan 15;71(2):506-15. PubMed PMID: 21084274.
- Tse C, Shoemaker AR, Adickes J, Anderson MG, Chen J, Jin S, Johnson EF, Marsh KC, Mitten MJ, Nimmer P, Roberts L, Tahir SK, Xiao Y, Yang X, Zhang H, Fesik S, Rosenberg SH, Elmore SW (2008). ABT-263: a potent and orally bioavailable Bcl-2 family inhibitor. Cancer Res. May 1;68(9):3421-8. PubMed PMID: 18451170.
- Zantl N, Weirich G, Zall H, Seiffert BM, Fischer SF, Kirschnek S, Hartmann C, Fritsch RM, Gillissen B, Daniel PT, Häcker G (2007). Frequent loss of expression of the pro-apoptotic protein Bim in renal cell carcinoma: evidence for contribution to apoptosis resistance. Oncogene. Oct 25;26(49):7038-48. PubMed PMID: 17486061.
- Zhu S, Cohen MB, Bjorge JD, Mier JW, Cho DC (2013). PI3K inhibition potentiates Bcl-2-dependent apoptosis in renal carcinoma cells. J Cell Mol Med. 2013 Mar;17(3):377-85. PubMed PMID: 23387989.
|
|
Letter: Budget cuts threaten life-saving dialysis treatment - The State Journal-Register |
The State Journal-Register
I am a nurse at a dialysis clinic that provides life-sustaining treatment for people with kidney failure. I am worried the proposed state budget cuts for Medicaid severely will impact the patients I serve every day. There are 18,000 people with kidney
|
|
DaVita expands renal, diabetes clinical trial services in EU - OutSourcing-Pharma.com |
|
Thanks to the expansion, which will include the addition of 10 physician leaders across the three countries, DaVita will be able to conduct late phase clinical trials outside of the US for the first time.
Amy Young, VP and general manager of DaVita Clinical Research, told Outsourcing-Pharma.com that the expansion in Europe will include renal and diabetes clinical trials.
"Combining extensive nephrology and clinical trial experience with knowledge of local differences in the practice of nephrology positions us as a valuable resource in drug development for chronic kidney disease management," Young added.
In addition to the new work in Europe, DaVita previously conducted Phase I clinical trials in the US since 1985, expanding its capabilities to include late phase clinical research, real-world health care data, health economics and outcomes research and medical communications. The company says it has helped to develop every end stage renal disease drug approved by the US FDA over the last 15 years.
“There is increasing demand for global clinical trials,” Young said. “The ability to provide access in many different countries via a central point of contact, like DaVita Clinical Research, is valuable and desirable for drug and device developers.”
|
|
Bobby's renal reality - The Young Witness |
|
Bobby Sims was 22 and working as a shearer in the back country when he was diagnosed with incurable polycystic kidney disease. His doctor’s advice was to go and enjoy life.

KICKED?IN?THE?GUTS:?“I’ve got no problems with Cowra getting a unit but why should those helping us go over the boundary fence and help others?” Bobby Sims at Young’s self managed renal unit this week.
Bobby Sims was 22 and working as a shearer in the back country when he was diagnosed with incurable polycystic kidney disease. His doctor’s advice was to go and enjoy life.
Eleven years later he started dialysis. He had both kidneys removed at 36. Had a kidney transplant at 45. That failed. He’s now 55.
Every day of his life for the past 33 years Bobby’s had to watch what he eats and drinks and every other day he has to manually remove the waste from his body.
He’s pretty much done it all; the trips to Canberra that sometimes took two days to return from, he’s self managed at home, he’s used manual bags. He’s also seen the quiet deterioration of other patients who have been on the same journey. Some of them are now dead.
Nowadays Bobby spends up to six hours three days a week holed up at Young’s self managed renal unit located at the western edge of the Young District Hospital compound - his right arm and leg have pronounced gortex loops that allow him to insert large needles that remove the waste from his body at a rate of 500 ml per hour.
The self managed unit was funded through a $120,000 community fundraising effort and $75,000 from NSW Health, opening to patients in November 2011.
At the time Bobby was the only patient using it and he said it allowed him to spend more time with his family. He said his life was halfway to normal.
Now, life isn’t so normal. His health’s deterioriating and his body is starting to wear out.
He’s had a couple of scares where he’s been choppered over to Canberra - the last time his lungs were full of fluid and he couldn’t breathe.
“I called 000, ran the blood back into my body and then blacked out - three hours later I woke up in emergency in Canberra Hospital,” he said.
Bobby thinks he’ll soon have to join the other patients who leave Young by bus at 4.30am three days a week to journey to Canberra for dialysis.
But it means he can have four litres of fluid removed in four hours.
He says the trips to Canberra take their toll.
“It’s hard on them,” he said, “they start out all chirpy and by the end of 12 months they have aged considerably.
“I’ve been on that bus and even have saved a few patients who passed out because they’ve had too much fluid taken out of their body,” he said.
The recent reversal of the decision to house a managed renal unit in Young has been, to Bobby, like a kick in the guts.
“There was a meeting four years ago and we were promised a unit, so I feel like we’ve been stabbed in the back - they may as well line us up and shoot us now,” he said.
“I’ve got no problems with Cowra getting a unit but why should those helping us go over the boundary fence and help others,” he asked.
He was the first to raise the alarm in Young. He tried to speak to Nationals Senator Fiona Nash and said the first person he encountered tried to rip down everything he said.
“But two days later Senator Nash called back and said she would be sending a letter to Katrina Hodgkinson and the state health minister on my behalf,” he said.
“I’ve written to a lot of politicians in my time and it’s the first time I’ve got an answer,” he said.
He cannot understand why every town in Victoria has a renal unit and are funding a Big Red Kidney Bus to allow dialysis patients to take holidays.
“The state government supports them better than us,” he said.
He doesn’t mince words either. He’d be more than happy to see the person who decided not to allow Young a managed renal unit to suffer kidney failure and live life hooked up to a dialysis machine.
“That’s what I want,” he said.
And he hopes the Young community gets behind the petition circulating around town.
“I think it’s a great thing to have this support for our cause and I want to thank the council for getting behind it and all the local people in town for helping us out,” he said.
He was particularly thankful to Mark Sheridan and Frank Baker for all they have done to get support for renal patients in Young. And he’s disappointed all their efforts of late have come to naught.
“We were told we were getting it by the people running the show and we were waiting for the final ok - even people in Canberra are telling us we need a renal unit - and this happens,” he said.
“I wish the powers that be would get their act together and they would listen to us and give us what we need,” Bobby said.
|
|
|
 Log in to explore the world's most comprehensive database of dialysis centres for free!
Log in to explore the world's most comprehensive database of dialysis centres for free!